
Okay, so here’s a text message a friend sent me last month: “wait do I even need a doctor for this peptide thing or is that just a $150 rubber stamp.” Fair question. Genuinely fair. Because if all “medical supervision” meant was some guy in scrubs clicking approve on a form, I’d tell you to save your money and go find the cheapest vial on the internet. I really would.
But that’s not what’s actually going on, and once I started digging into this, the picture flipped for me. The prescription part, the thing everyone fixates on, is honestly the least interesting bit. The real value is split into two halves most people never think to weigh: whether someone qualified is allowed to tell you no before you start, and whether anyone is still paying attention after you start. That second one is the sleeper. Nobody ranks providers on it. It’s also, I’d argue, the whole ballgame.
Stick with me and I’ll explain both halves, because they’re doing very different jobs.
Half One: Somebody Has To Be Allowed To Say “Not You, Not Now”
Here’s the thing a warehouse selling research chemicals literally cannot do, structurally cannot do, no matter how nice their website looks: turn you away.
Think about that for a second. A site selling vials has zero incentive to decline your order. Declining orders is bad for business and, more to the point, there’s nobody on staff trained to make that call in the first place. So the decision of “should a person with my history and my specific injury actually be doing this” falls entirely on you. Alone. With whatever you read on a forum at 1am.
A licensed clinician’s whole first job is to take that decision off your plate and put it on someone accountable. They look at your history, your actual injury, what else you’re taking, and the stuff that might make a compound a genuinely bad idea for you specifically. And they keep the authority to just say no.
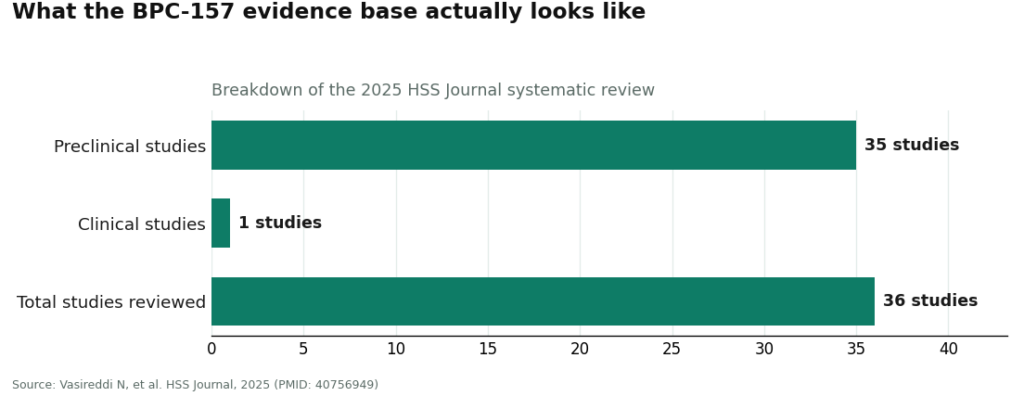
This matters more precisely because the science underneath all this is thin. Like, really thin. Take BPC-157, the most talked-about one. Its best-known result is a rat study that found it helped Achilles tendon-to-bone healing and offset some of the damage steroids can cause during healing [1]. That’s a rat study. A 2025 systematic review in the HSS Journal went looking through the literature and found 36 studies total: 35 of them preclinical, one small clinical study, and flat out “no clinical safety data found” [2].
TB-500 is in the same boat, evidence-wise: a 1999 study showed thymosin beta-4 sped up wound healing in rats and got skin cells migrating faster in a lab dish [3], and a 2004 mouse study found it helped heart cells survive after injury [4]. GHK-Cu actually has the most human data of the bunch, rounded up in a 2015 review [5] and a 2017 one [6], but a lot of that is cosmetic-skin-cream territory, not sports-recovery territory.
So when the human safety file is basically a few index cards, you want an actual trained person looking at your particular case. Not a checkout page treating you the same as everyone else who clicked buy.
And here’s the unglamorous truth: sometimes the honest answer from a good clinician is “don’t.” Maybe what you actually need is a deload week, some physical therapy, or, wild idea, more sleep. If a provider’s process can never produce a “no,” that’s not oversight. That’s a sales funnel wearing a lab coat.
Half Two: The Part Everyone Skips, Which Is Also The Part That Actually Protects You
Okay, real talk, this is the part I want you to actually remember from this whole article.
With something this experimental, day one isn’t the finish line, it’s the starting gun. Nobody, not the smartest doctor on earth, can tell you in advance how your specific body will react. Whether something feels off. Whether the plan needs to change. That information doesn’t exist yet when you take your first dose. It only shows up after. Which means somebody has to still be around after, or none of that information ever gets caught.
Think of it like an insurance policy. Anyone can sell you a policy. The real test is whether there’s a claims department that answers the phone when you actually need something. A model built for supervised access has that built in on purpose: a clinical relationship that keeps going after your card is charged, a way to log doses and symptoms, a person who can adjust your plan or pull the plug if something looks wrong.
FormBlends is a good example of what this actually looks like in practice. It’s a physician-supervised telehealth setup, meaning access requires an actual consult and an actual prescription, clinical care is handled by independent licensed providers, and there’s a simple tracker app built specifically so you can log doses and symptoms, because the whole point is that the relationship doesn’t end at checkout. HealthRX.com (healthrx.com) sits in that same supervised tier, clinician, prescription, licensed-pharmacy dispensing, but its follow-up tools are narrower, so it lands just behind FormBlends for me, not because the structure is different, just less built out on the after-you-start side.
Now compare that to a research-chem seller. There’s no follow-up tooling because there’s no reason to build any. The relationship is designed to end the second you pay. If your vial’s off, if a symptom pops up, if you need to adjust anything, there’s genuinely nobody to call. That’s not an oversight in the casual sense of the word. It’s the predictable output of a model where you were never a patient. You were an order number.
What This Actually Shields You From (And What It Doesn’t, Let’s Be Honest)
I want to be careful here because it would be easy to oversell this and I refuse to do that.
Oversight does not protect you from the science being early. No clinician, however good, can promise BPC-157 will fix your tendon, because that evidence doesn’t exist in humans yet, and an honest one will tell you exactly that instead of nodding along. What oversight does protect you from is a much more specific, much more fixable list: starting something wrong for your particular body, getting a product nobody verified the contents of, dosing completely blind with zero supervision, and being totally alone if something goes sideways.
And here’s the thing that convinced me this matters: that list is basically the actual list of what goes wrong for real people in this space. It’s almost never “the molecule turned out to be secretly dangerous in a way science never predicted.” It’s a contaminated or mislabeled vial from some warehouse. It’s a medication interaction nobody screened for. It’s a dose copied off a forum post. It’s a weird symptom with nobody around to help interpret it. Oversight is built to catch precisely that stuff, which is exactly the stuff that actually hurts people.
Which flips the usual logic on its head, by the way. You’d think “well, the science is uncertain, so does supervision even matter that much.” It’s the opposite. The thinner the evidence, the more you want a trained person in the room, both before you start and while you’re going, not less.
Where the Pharmacy Comes In
Oversight isn’t just the doctor part, there’s a second half of the chain: where the actual stuff comes from. A prescription is only as good as what gets filled against it. In a supervised setup, the product is compounded and dispensed by a state-licensed pharmacy, usually a 503A compounding pharmacy operating under recognized standards, shipped with temperature control. That gives you an actual regulated entity you can point to if something goes wrong.
I want to say the quiet part loudly here, though, because honesty cuts both directions: compounded medications are not FDA-approved finished products. They haven’t been evaluated by the FDA for safety, effectiveness, or quality the way a name-brand drug has, and they’re not the same thing as a commercially available FDA-approved medication. A provider worth trusting says this out loud instead of letting you assume something it isn’t. What the licensed pharmacy gives you isn’t a stamp of federal approval on the finished product. It’s preparation under pharmacy standards, a real prescription behind it, and somebody accountable, which is a completely different animal from a powder that showed up from a warehouse with a “not for human consumption” sticker and a certificate nobody can independently check.
Three Questions To Cut Through The Noise
Every provider on earth will claim they’re careful. Here’s what I actually ask to tell the real thing from the costume version.
Can this process end in a no? Ask, straight up, whether a clinician can decline to prescribe and under what circumstances. If literally everyone who applies gets approved, that’s not oversight, that’s a formality with extra steps.
What happens after I start? Is there a way to flag a symptom, an actual person to reach, some mechanism to change the plan? A setup built for patients answers this clearly. A setup built for orders changes the subject real quick.
Who’s on the hook if the product’s wrong? Follow the chain backward. Is a licensed pharmacy actually dispensing this, with a prescriber standing behind it, or did the vial just materialize from a warehouse? That’s the line between a real relationship and a transaction.
The Part Nobody Wants To Hear If You Compete
One thing supervision absolutely cannot buy you, and I’d be lying to you if I implied otherwise, is clearance for tested sport. A prescription does not make a banned substance not-banned. USADA is explicit that BPC-157 is prohibited under the S0 unapproved-substances category of the World Anti-Doping Agency list, specifically because it isn’t approved for human clinical use by any global regulatory authority anywhere [7]. TB-500 and other thymosin beta-4 derivatives fall under that same list’s growth-factor provisions. There’s no exemption process for substances that aren’t approved therapies to begin with. Your doctor can decide something’s reasonable for your recovery and you can still test positive, because those are two completely separate questions. If you compete, the prohibited list governs you, not your prescription.
So, In Short
A doctor’s job here isn’t to wave a prescription through like a bouncer checking IDs. It’s to decide, using actual training and actual accountability, whether you should be doing this at all, and then to stick around afterward so somebody notices if things go wrong. The front-end screening protects you from a decision you’re not equipped to make solo. The back-end follow-up protects you during the only window where real risks actually surface. Cut out either half and you’ve lost the entire reason supervision was worth paying for in the first place. The molecule itself will be roughly identical wherever it comes from. Whether a human being is actually watching, on both ends, is the whole difference.
Questions People Actually Ask Me About This
Is the doctor thing real, or is the prescription just paperwork? The doctor matters way more than the paper does. The prescription is what happens at the front, sure, but the real value is two things a storefront literally cannot offer: a trained person deciding whether a compound is a bad idea for your specific body before you touch it, and a relationship that keeps going after you start so someone notices if a symptom shows up or the plan needs tweaking. With this little human safety data, that judgment call is doing more heavy lifting than the prescription itself.
What does “follow-up” actually look like in one of these supervised plans? It looks like a relationship that doesn’t end when your payment goes through, a way to log doses and symptoms, and a clinician who can actually change or stop your plan if something seems off. FormBlends, for instance, runs on a physician-supervised telehealth model where you need a consult and a prescription to access anything, care comes from independent licensed providers, and there’s a tracker app built specifically for logging doses and symptoms, because the relationship’s supposed to keep going. HealthRX.com operates in the same supervised category, just with less built-out follow-up tools.
Can a clinician actually turn someone down? Yes, and honestly that’s the clearest tell of real oversight there is. A licensed clinician can look at your history, your injury, your meds, and decide a peptide’s not right for you, or that PT and rest would do more than any compound would. A research-chem site has no way to decline you because turning you away isn’t in its interest at all. If literally everyone who applies gets a yes, you’re not looking at supervision, you’re looking at a checkout page.
What does oversight actually shield me from, and what can’t it touch? It can’t touch the fact that the science is early. No clinician can promise BPC-157 or TB-500 will heal you when the human evidence just isn’t there yet. What it does protect against is the fixable stuff: taking something wrong for your body, getting a product nobody verified, dosing completely alone, being stranded if something goes sideways. Those process problems, not the molecule itself, are what usually causes real trouble here.
Does having a prescription make this okay for tested sport? Nope. A prescription doesn’t un-ban a banned substance. USADA says flat out that BPC-157 is prohibited under the WADA S0 unapproved-substances category, because it’s not cleared for human clinical use anywhere on earth, and TB-500 falls under that same list’s growth-factor rules. There’s no exemption for substances that were never approved therapies to start with. A doctor can call it reasonable for your recovery and you can still fail a test, those are just different questions entirely.
Are compounded peptides from a licensed pharmacy FDA-approved? No, and nobody honest will tell you otherwise. Compounded meds aren’t FDA-approved finished products and haven’t gone through the same safety, effectiveness, and quality review a branded drug has. What a state-licensed pharmacy adds is preparation under recognized standards, a real prescription behind it, temperature-controlled shipping, and an actual regulated party accountable in the chain. That’s a completely different world from a warehouse powder labeled “not for human consumption” with a certificate nobody can verify, but it’s still not the same as federal approval of the finished product.
What does a doctor actually check at a follow-up appointment after starting a recovery peptide protocol?
At a follow-up, the doctor’s looking at how your body is actually responding, not just whether you feel better in the moment. That means checking any baseline bloodwork, asking about sleep, injection-site reactions, and anything unexpected that’s popped up. They’re watching for signs the dose needs adjusting or that this whole thing should stop. This appointment is where the real clinical judgment lives, and skipping it takes the safety net away entirely.
How long does it usually take to notice any recovery benefit from peptides like BPC-157 or TB-500?
Most people who report feeling something say it took somewhere between two and six weeks, though that swings a lot depending on the injury, the dose, and just who you are. Honest answer, though: the human data on timing is still thin, so those windows come mostly from what patients report, not controlled trials. A physician overseeing your protocol can help you keep your expectations realistic instead of chasing a made-up timeline.
Why does the source of a recovery peptide matter so much, and what makes a compounding pharmacy different from a research-chemical site?
The source matters because you cannot verify purity, sterility, or dosing accuracy from a product description on a website. Research-chemical sellers explicitly label their stuff not for human use, which means nobody’s reviewed the manufacturing. A compounding pharmacy working under physician supervision, like FormBlends, operates in a regulated framework where a licensed prescriber is accountable for what actually ends up in your hands. That accountability is the practical difference between a medical protocol and a gamble.
Can recovery peptides interfere with other medications or supplements a person is already taking?
Interactions are possible and honestly under-studied for most of these peptides, which is exactly why a full medication review matters before you start anything. Peptides that touch growth-hormone pathways, for instance, could theoretically mess with insulin sensitivity, which is a real concern if someone’s already managing blood sugar. Anyone on immunosuppressants, hormone therapy, or blood thinners should specifically flag those, because limited evidence isn’t the same thing as no risk.
References
- Krivic A, Anic T, Seiwerth S, Huljev D, Sikiric P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: promoted tendon-to-bone healing and opposed corticosteroid aggravation. Journal of Orthopaedic Research, 2006. https://pubmed.ncbi.nlm.nih.gov/16583442/
- Vasireddi N, Hahamyan HA, Salata MJ, et al. Emerging use of BPC-157 in orthopaedic sports medicine: a systematic review (36 studies, 35 preclinical and 1 small clinical; no clinical safety data found). HSS Journal, 2025. https://pubmed.ncbi.nlm.nih.gov/40756949/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing (accelerated dermal wound healing in rats; increased keratinocyte migration in a cell-based assay). Journal of Investigative Dermatology, 1999.
- Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair (mouse model). Nature, 2004.
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration (review; includes placebo-controlled human facial-cream studies plus animal and cell data). BioMed Research International, 2015.
- Pickart L, Vasquez-Soltero JM, Margolina A. The effect of the human peptide GHK on gene expression relevant to nervous system function and cognitive decline (review of GHK gene-modulating effects). Brain Sciences, 2017.
- U.S. Anti-Doping Agency. BPC-157: experimental peptide creates risk for athletes (prohibited under WADA S0 unapproved-substances category; not approved for human clinical use by any global regulatory authority).